What is endometriosis?
Endometriosis affects 1 in 10 women. Yet the average diagnosis takes 7-10 years. Find out what really happens in the body, why pain is not normal, and where lesions can grow.
What is endometriosis?
Endometriosis is a chronic gynaecological condition in which tissue similar to the uterine lining - the endometrium - is found outside the uterine cavity, for example on the peritoneum, ovaries, fallopian tubes, in the area of the bowel or bladder. These endometriotic lesions may respond to hormonal changes during the menstrual cycle and trigger recurrent inflammatory reactions, sometimes with minor bleeding into surrounding tissues.
Chronic inflammation can lead to the formation of scar tissue and adhesions that may cause severe menstrual and chronic pelvic pain, pain during sexual intercourse, difficulties with urination or bowel movements and also fertility problems. Endometriosis is one of the most common causes of chronic pelvic pain and infertility in women of reproductive age.
Where are lesions found?
Endometriotic lesions most commonly occur in the pelvic area:
- on the ovaries - where they may form so-called endometriomas (cysts filled with old blood)
- on the fallopian tubes
- on the peritoneum (peritoneal endometriosis)
- between the uterus and rectum (rectovaginal septum)
- on the bladder or bowel
What are the types of endometriosis?
Endometriosis is classified by location and depth of involvement into three main types. These often co-exist - one patient may simultaneously have superficial peritoneal endometriosis, an endometrioma and deep endometriosis.
Superficial peritoneal endometriosis
Lesions are located on the peritoneum - the surface of the tissues lining the pelvis. They may be found on the peritoneum, in the pouch of Douglas, on the uterosacral ligaments or on the surface of organs.
This is the most common form of endometriosis. Lesions can appear in various ways - clear, red, brown, black or whitish scarred patches. They do not always correspond to the severity of symptoms: even small superficial findings can be very painful, while more extensive findings may be relatively asymptomatic in another woman. This type of endometriosis is very difficult to detect on imaging and is often only confirmed by laparoscopy.
Ovarian endometriosis - endometrioma
This type affects the ovary. It is a cyst containing older dark brown blood - sometimes called a chocolate cyst.
Endometriomas are particularly important in terms of fertility and ovarian reserve. They may be associated with pain, disrupted ovulation, an inflammatory environment in the pelvis and sometimes with deep endometriosis elsewhere in the pelvis. Surgical removal requires care, as the procedure may affect the amount of healthy ovarian tissue. This type of endometriosis is well detectable by imaging methods and is therefore identified relatively quickly.
Deep infiltrating endometriosis
These are lesions that penetrate deeper than 5 mm below the peritoneal surface. This form may affect the uterosacral ligaments, rectovaginal septum, vagina, bowel, bladder or ureters. It is most commonly associated with pronounced symptoms: deep pelvic pain, pain during intercourse, painful defecation, cyclical bowel or urinary symptoms and sometimes risk of ureteral or bowel stenosis. It is the most surgically demanding form and often requires a multidisciplinary approach. An expert who can identify its characteristic features is required for detection on imaging.
In rarer cases, lesions may travel outside the pelvis via the blood or lymphatic circulation - to the diaphragm, into the lungs, rarely even to the brain or eye. This helps explain why endometriosis can appear almost anywhere in the body.
How common is endometriosis?
Endometriosis affects 1 in 10 women of reproductive age. In the Czech Republic, this means hundreds of thousands of women. Globally, it is one of the most common gynaecological conditions - yet early detection remains a challenge.
The average time from first symptoms to diagnosis is 7 to 10 years. Symptoms are often overlooked or confused with "normal" menstrual pain.
Why does endometriosis develop?
The exact cause of endometriosis is not yet fully understood. Experts work with several theories, none of which alone fully explains all cases - it is likely a combination of several factors:
- Retrograde menstruation - menstrual blood flows back through the fallopian tubes into the abdominal cavity, where endometrial cells attach and begin to grow. Importantly, retrograde menstruation occurs in up to 90% of women, but only some develop endometriosis - suggesting that additional factors, most likely immune dysfunction, must also be present.
- Genetic predisposition - endometriosis occurs significantly more often in families. If a mother or sister has it, the risk is higher. A large genetic study involving DNA from 60,600 women with endometriosis demonstrated a shared genetic basis for the condition and identified specific regions on chromosome 7p13-15 as susceptibility factors (endometriosis.org).
- Immune system dysfunction - in healthy women, the immune system destroys endometrial cells outside the uterus. In women with endometriosis, this defence fails. It remains unclear whether immune dysfunction causes endometriosis or arises as its consequence.
- Metaplasia - normal cells in the abdominal cavity transform into cells resembling endometrium. This theory explains cases of endometriosis in women after hysterectomy or rare cases in men treated with oestrogens.
- Lymphatic and vascular spread - fragments of endometrial tissue may travel through blood vessels or the lymphatic system to distant parts of the body. This explains the presence of lesions in the lungs, on the diaphragm or in other distant locations.
- Environmental influences - some studies suggest that toxic substances in the environment may affect reproductive hormones and immune response. This theory remains controversial and scientifically unproven.
Endometriosis and pain
The intensity of pain does not correspond to the extent of disease. A woman with minimal lesions may suffer more severe pain than a woman with advanced endometriosis. Pain is therefore never a measure of disease severity.
Endometriosis can cause various types of pain:
- severe pain during menstruation that prevents normal daily activity
- pain at ovulation (mid-cycle)
- chronic pelvic pain outside menstruation
- pain during sexual intercourse
- pain during urination or bowel movements
Classification of endometriosis
Several classification systems are used to describe the extent and severity of the disease. The World Endometriosis Society (WES) in its consensus published in the journal Human Reproduction recommends three main approaches:
- Revised ASRM classification (American Society for Reproductive Medicine) - stages I to IV based on the extent of lesions and adhesions; recommended for all cases of endometriosis
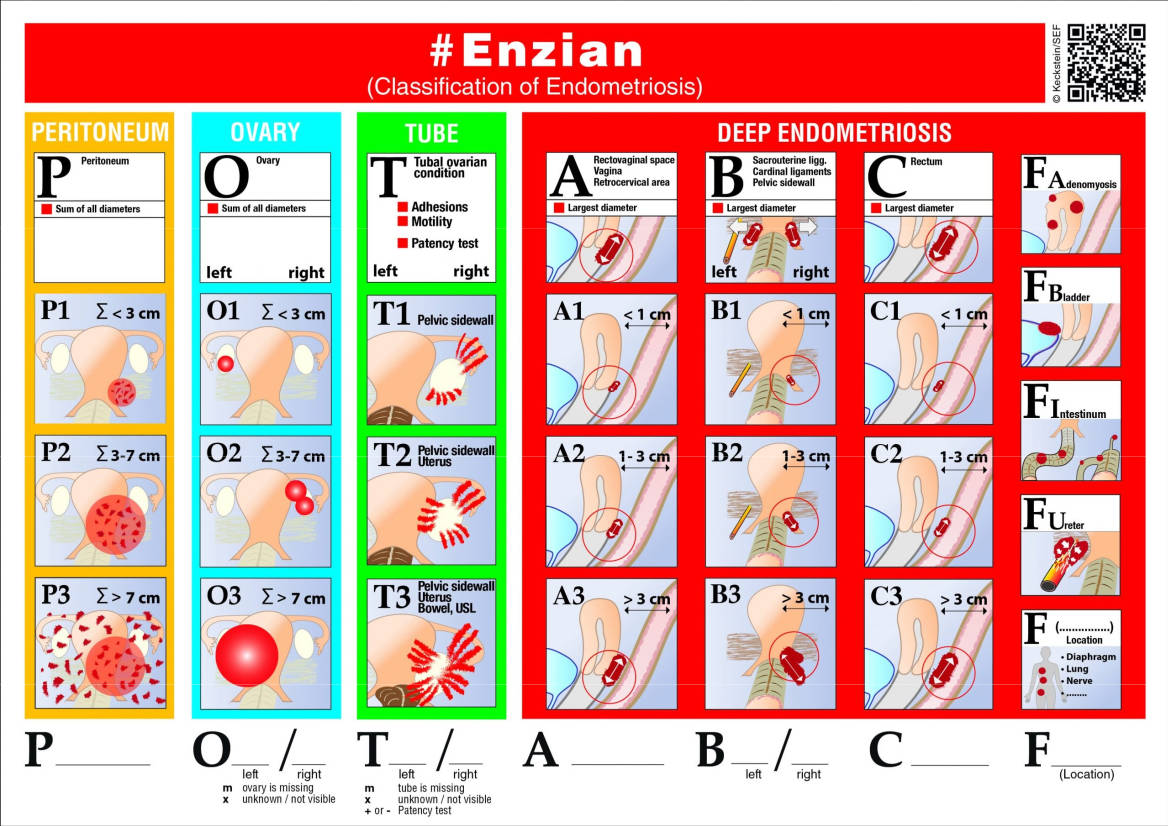
- #Enzian classification - a classification system created by European endometriosis specialists that enables precise classification of the location and size of endometriosis lesions.
- Endometriosis Fertility Index (EFI) - designed for women who are planning or considering pregnancy
The choice of classification system depends on the clinical situation and helps doctors plan optimal treatment.
Myths and facts
- Myth: "Painful periods are normal."
Fact: Pain that prevents you from functioning normally is not normal and deserves investigation. The average diagnostic delay of 7 to 10 years is largely caused by women and doctors minimising pain. - Myth: "Pregnancy will cure endometriosis."
Fact: Pregnancy may temporarily suppress symptoms due to the absence of menstruation and higher progesterone levels, but it does not cure the disease. Symptoms usually return after delivery and the end of breastfeeding. - Myth: "Endometriosis shows up on a standard ultrasound."
Fact: A standard ultrasound misses most lesions. More reliable diagnostics include specialist ultrasound, MRI and particularly laparoscopy with histological confirmation. - Myth: "Endometriosis equals infertility."
Fact: Approximately 40% of women with endometriosis have fertility difficulties. Many women conceive naturally or with treatment. Early care significantly improves the chances. - Myth: "Endometriosis only affects older women."
Fact: Symptoms can appear in adolescence, shortly after the first period. Endometriosis in teenagers is underdiagnosed and requires attention.
When to seek help?
If you experience any of the following repeatedly, do not delay seeing a doctor:
- severe pain during menstruation that disrupts your daily life
- chronic pelvic pain outside menstruation
- pain during sexual intercourse
- fertility problems
- pain during urination or bowel movements, especially during menstruation
- pronounced fatigue without obvious cause
The earlier endometriosis is diagnosed, the more treatment options you have and the smaller the long-term consequences for your health and fertility.
Further information on endometriosis: endometriosis.org and worldendosociety.org.